Colorectal Cancer Prevention (PDQ®): Prevention - Patient Information [NCI]
General Information About Colorectal Cancer
Colorectal cancer is a disease in which malignant (cancer) cells form in the tissues of the colon or the rectum.
The colon is part of the body's digestive system. The digestive system removes and processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) from foods and helps pass waste material out of the body. The digestive system is made up of the mouth, throat, esophagus, stomach, and the small and large intestines. The colon (large bowel) is the first part of the large intestine and is about 5 feet long. Together, the rectum and anal canal make up the last part of the large intestine and are 6 to 8 inches long. The anal canal ends at the anus (the opening of the large intestine to the outside of the body). 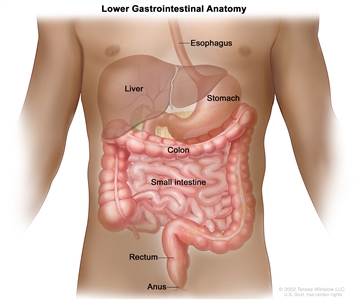
Anatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
Cancer that begins in the colon is called colon cancer, and cancer that begins in the rectum is called rectal cancer. Cancer that affects either of these organs may also be called colorectal cancer.
See the following PDQ summaries for more information about colorectal cancer:
- Colorectal Cancer Screening
- Colon Cancer Treatment
- Rectal Cancer Treatment
- Genetics of Colorectal Cancer
Colorectal cancer is the third leading cause of death from cancer in the United States.
Between 2011 and 2019, the number of new colorectal cancer cases in the United States decreased slightly per year in people aged 50 years and older, but increased slightly per year in people younger than 50 years. For the past 20 years, the rate of deaths from colorectal cancer has been decreasing in both men and women. The number of new cases and the number of deaths are higher in Black people compared with other races; however, studies have found no evidence that Black people have higher rates of precancerous lesions.
Finding and treating colorectal cancer early may prevent death from colorectal cancer. Screening tests may be used to help find colorectal cancer.
Colorectal Cancer Prevention
Avoiding risk factors and increasing protective factors may help prevent cancer.
Avoiding cancer risk factors may help prevent certain cancers. Risk factors include smoking, being overweight, and not getting enough exercise. Increasing protective factors such as quitting smoking and exercising may also help prevent some cancers. Talk to your doctor or other health care professional about how you might lower your risk of cancer.
The following risk factors increase the risk of colorectal cancer:
Age
The risk of colorectal cancer increases after age 50. Most cases of colorectal cancer are diagnosed after age 50.
Family history of colorectal cancer
Having a parent, brother, sister, or child with colorectal cancer doubles a person's risk of colorectal cancer.
Personal history
Having a personal history of the following conditions increases the risk of colorectal cancer:
- Previous colorectal cancer.
- High-risk adenomas (colorectal polyps that are 1 centimeter or larger in size or that have cells that look abnormal under a microscope).
- Ovarian cancer.
- Inflammatory bowel disease (such as ulcerative colitis or Crohn disease).
Inherited risk
The risk of colorectal cancer is increased when certain gene changes linked to familial adenomatous polyposis (FAP) or hereditary nonpolyposis colon cancer (HNPCC or Lynch Syndrome) are inherited.
Alcohol
Drinking 3 or more alcoholic beverages per day increases the risk of colorectal cancer. Drinking alcohol is also linked to the risk of forming large colorectal adenomas (benign tumors).
Cigarette smoking
Cigarette smoking is linked to an increased risk of colorectal cancer and death from colorectal cancer.
Smoking cigarettes is also linked to an increased risk of forming colorectal adenomas. Cigarette smokers who have had surgery to remove colorectal adenomas are at an increased risk for the adenomas to recur (come back).
Race
Black individuals have an increased risk of colorectal cancer and death from colorectal cancer compared to other races.
Obesity
Obesity is linked to an increased risk of colorectal cancer and death from colorectal cancer.
The following protective factors decrease the risk of colorectal cancer:
Physical activity
A lifestyle that includes regular physical activity is linked to a decreased risk of colorectal cancer.
Aspirin
Studies have shown that taking aspirin daily for at least two years lowers the risk of colorectal cancer and the risk of death from colorectal cancer. The decrease in risk begins 10 to 20 years after patients start taking aspirin.
The possible harms of aspirin use (100 mg or less) daily or every other day include an increased risk of stroke and bleeding in the stomach and intestines. These risks may be greater among the elderly, men, and those with conditions linked to a higher than normal risk of bleeding.
Combination hormone replacement therapy
Studies have shown that combination hormone replacement therapy (HRT) that includes both estrogen and progestin lowers the risk of invasive colorectal cancer in postmenopausal women.
However, in women who take combination HRT and do develop colorectal cancer, the cancer is more likely to be advanced when it is diagnosed and the risk of dying from colorectal cancer is not decreased.
The possible harms of combination HRT include an increased risk of having:
- Breast cancer.
- Heart disease.
- Blood clots.
Polyp removal
Most colorectal polyps are adenomas, which may develop into cancer. Removing colorectal polyps that are larger than 1 centimeter (pea-sized) may lower the risk of colorectal cancer. It is not known if removing smaller polyps lowers the risk of colorectal cancer.
The possible harms of polyp removal during colonoscopy or sigmoidoscopy include a tear in the wall of the colon and bleeding.
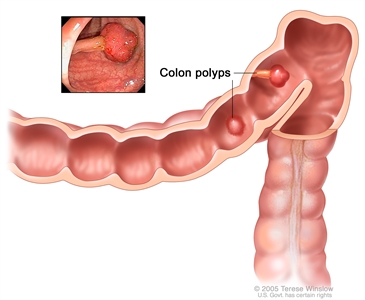
Polyps in the colon. Some polyps have a stalk and others do not. Inset shows a photo of a polyp with a stalk.
It is not clear if the following affect the risk of colorectal cancer:
Nonsteroidal anti-inflammatory drugs (NSAIDs) other than aspirin
It is not known if the use of nonsteroidal anti-inflammatory drugs or NSAIDs (such as sulindac, celecoxib, naproxen, and ibuprofen) lowers the risk of colorectal cancer.
Studies have shown that taking the nonsteroidal anti-inflammatory drug celecoxib reduces the risk of colorectal adenomas (benign tumors) coming back after they have been removed. It is not clear if this results in a lower risk of colorectal cancer.
Taking sulindac or celecoxib has been shown to reduce the number and size of polyps that form in the colon and rectum of people with familial adenomatous polyposis (FAP). It is not clear if this results in a lower risk of colorectal cancer.
The possible harms of NSAIDs include:
- Kidney problems.
- Bleeding in the stomach, intestines, or brain.
- Heart problems such as heart attack and congestive heart failure.
Calcium
It is not known if taking calcium supplements lowers the risk of colorectal cancer.
Diet
It is not known if a diet low in fat and meat and high in fiber, fruits, and vegetables lowers the risk of colorectal cancer.
Some studies have shown that a diet high in fat, proteins, calories, and meat increases the risk of colorectal cancer, but other studies have not.
The following factors do not affect the risk of colorectal cancer:
Hormone replacement therapy with estrogen only
Hormone replacement therapy with estrogen only does not lower the risk of having invasive colorectal cancer or the risk of dying from colorectal cancer.
Statins
Studies have shown that taking statins (drugs that lower cholesterol) does not increase or decrease the risk of colorectal cancer.
Cancer prevention clinical trials are used to study ways to prevent cancer.
Cancer prevention clinical trials are used to study ways to lower the risk of developing certain types of cancer. Some cancer prevention trials are conducted with healthy people who have not had cancer but who have an increased risk for cancer. Other prevention trials are conducted with people who have had cancer and are trying to prevent another cancer of the same type or to lower their chance of developing a new type of cancer. Other trials are done with healthy volunteers who are not known to have any risk factors for cancer.
The purpose of some cancer prevention clinical trials is to find out whether actions people take can prevent cancer. These may include exercising more or quitting smoking or taking certain medicines, vitamins, minerals, or food supplements.
New ways to prevent colorectal cancer are being studied in clinical trials.
Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.